
Everything You Need to Know About Your Dog's Cranial Cruciate Ligament (CCL).
- Samantha

- May 3
- 5 min read
Cranial cruciate ligament (CCL) disease is one of the most common causes of hindlimb lameness in dogs and a major contributor to chronic stifle pain and osteoarthritis (Vasseur, 2003; Comerford et al., 2011).
And despite what many people think, it usually isn’t caused by one dramatic injury.
Most of the time, it’s something that has been developing in your dog quietly over months or even years.
What is the Cranial Cruciate Ligament?
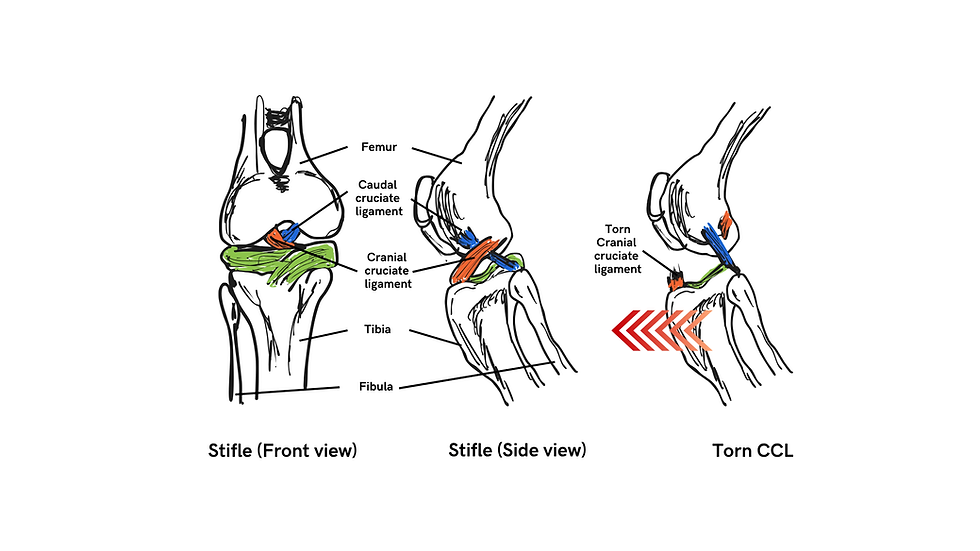
Similar to the human's anterior cruciate ligament (ACL), the dog's cranial cruciate ligament (CCL) keeps your dog’s knee (stifle joint) stable.
Its main roles are to help prevent:
the shin bone (tibia) from sliding forward
excessive twisting of the joint
hyperextension of the knee
It is one of the key stabilisers that keeps the knee stable during weight bearing movement such as walking, running and jumping (Pozzi et al., 2013). Any changes in this stability would affect the whole joint.
Myth: CCL disease only happen to very active dogs
While some dogs injure their CCL after a sudden slip, sharp turn, or awkward landing, most cases (approximately 80%) are actually due to gradual degeneration over time (Comerford et al., 2011).
This means that the ligament gradually weakens and eventually fails during a normal activity like:
Jumping off the sofa
Chasing a ball
Turning quickly
Stepping into a pot hole
That’s why many owners often say “They were completely fine yesterday!”. But little did they know that there was already an underlying progression of CCL disease.
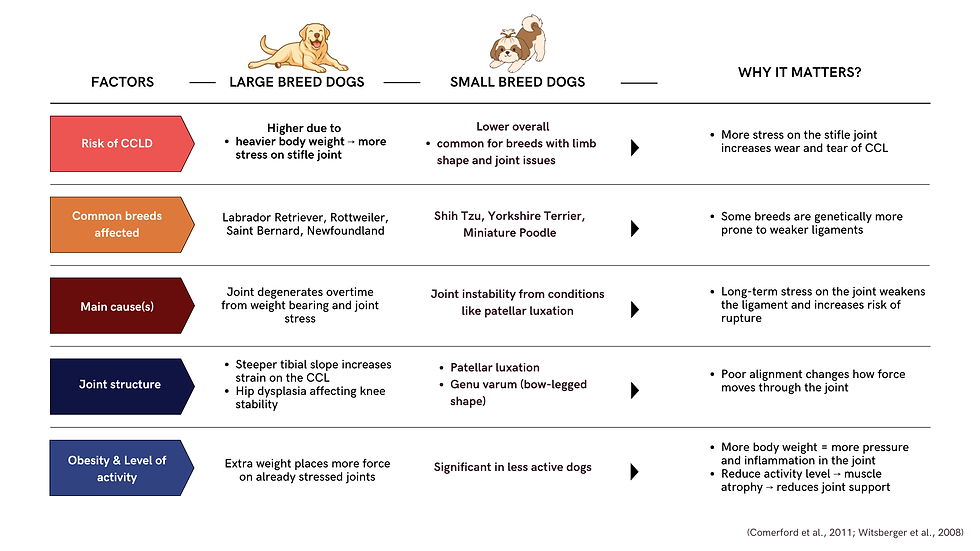
Predisposing Factors for CCL Disease
Common Signs Owners Notice
CCL disease often starts subtly.
Some early signs are:
“lazy sit” (sitting with one leg kicked out)
standing with more weight on one hindlimb
stiffness after rest
reluctance to jump or use stairs
difficulty getting up from lying down
gets tired more easily
less interest in play
limping or intermittent lameness
A combination of these signs together can suggest joint discomfort or instability. However, they are not specific to CCL injuries alone. It's always best to have your dog assessed by a veterinarian or an animal physiotherapist to get a clear idea of what is going on and guide your next steps. Schedule an appointment with us if you have any concerns.
Why It Matters
A CCL injury is not just a "ligament problem".
Because CCL plays a key role in stabilising the stifle (knee) joint, any damage to it affects how stable the joint is during movement. When the joint becomes less stable, small repeated micro-movements within the joint can occur even during everyday activities. Overtime, this may lead to:
Early degeneration of the meniscus or cartilage
Repeated joint inflammation which can progress to early arthritis
Muscle loss (especially the quadriceps), as pain and instability makes it harder to use their leg effectively
Therefore, early intervention is important. The longer instability continues, more damage and pain can develop, and the harder recovery becomes.
Surgical vs Conservative Management
Surgery is Generally the Gold Standard
Surgical stabilisation provides the best outcomes for:
restoring function
improving limb use
reducing instability
slowing progression of osteoarthritis (Christopher et al., 2013)
Common procedures include:

TPLO
(Tibial Plateau Levelling Osteotomy)
Changes stifle biomechanics by reducing cranial tibial thrust rather than replacing the ligament itself.
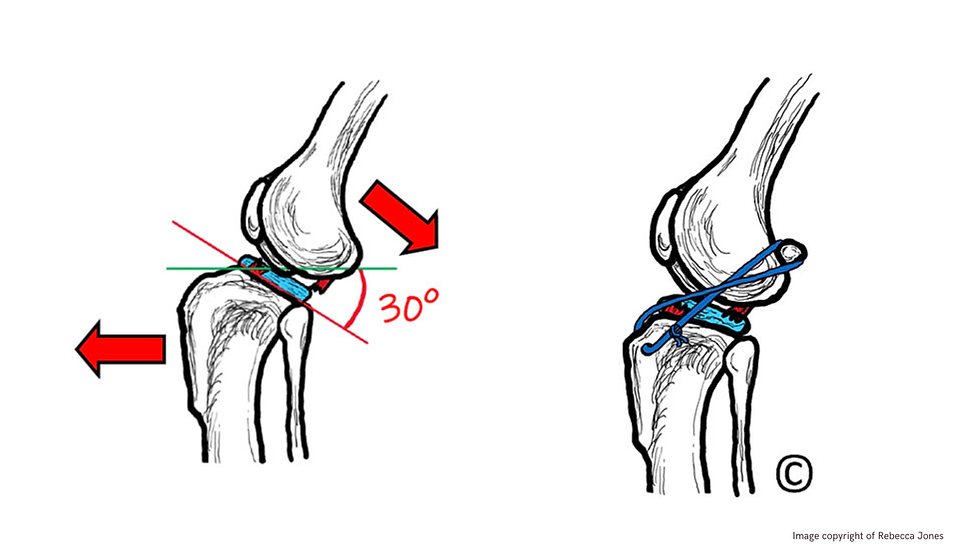
Lateral Fabellar Suture
(Extracapsular Stabilisation)
Provides passive stabilisation using a synthetic suture placed outside the joint.
Surgery is important and often necessary to correct the structural issue, but it is only the beginning of their recovery journey. Studies have shown dogs receiving post-op rehab perform better than dogs managed with crate rest alone (Marsolais et al., 2002).
Rehabilitation plays a key role in helping dogs rebuild strength in the surrounding muscles, regain confidence in weight-bearing on the affected leg and relearn a normal gait pattern.
Conservative Management
However, not all dogs may be eligible for surgery due to various reasons such as
advanced age
heart disease or anaesthetic risk
low activity level
financial limitations
owner preference
Therefore, conservative management (such as Physiotherapy) could be done to help manage the condition.
The Value of Physiotherapy
Rehabilitation is essential for both surgical and conservative (non-surgical) cases. Although the overall rehabilitation journey may be similar, the role of physiotherapy differs slightly depending on the management approach.
How physiotherapy helps your dog recover:

The Role of Physiotherapy in CCL rehabilitation (Surgical VS Conservative management)

Without proper rehabilitation, prolonged limping can lead to:
muscle wasting and weakness
reduced mobility
compensation injuries (overloading other limbs)
slower or incomplete recovery
How Can You Help Your Dog at Home?
Recovery doesn’t only happen during rehab sessions. What happens at home matters just as much.
Here are some simple changes you can make:
non-slip flooring or non-slip mats, especially in high traffic areas
avoid jumping on/off furniture
controlled leash walks
managing your dog's weight (BCS 4-5/9)
These small changes can make a meaningful difference to your dog. It supports their recovery and play an important role in managing their condition long-term.
Final Thoughts
CCL disease is one of the most common orthopaedic problems we see, but also one of the most manageable when caught early.
If your dog is:
limping
sitting strangely
slowing down
avoiding stairs
“just getting older”
It may be worth looking closer. Sometimes it’s not age. Sometimes it’s their knee asking for help.
References
Bleedorn JA, Greuel EN, Manley PA, et al. (2011). Synovitis in dogs with stable stifle joints and incipient cranial cruciate ligament rupture: a cross-sectional study. Veterinary Surgery, 40(5), 531–543.
Christopher SA, Beetem J, Cook JL. (2013). Comparison of long-term outcomes associated with three surgical techniques for treatment of cranial cruciate ligament disease in dogs. Veterinary Surgery, 42(3), 329–334.
Comerford EJ, Tarlton JF, Innes JF, et al. (2011). Metabolism and pathogenesis of canine cranial cruciate ligament disease. Veterinary Journal, 188(2), 141–148.
Johnson AL, Johnson JM. (1993). Cranial cruciate ligament rupture: pathogenesis, diagnosis, and postoperative rehabilitation. Veterinary Clinics of North America: Small Animal Practice, 23(4), 717–733.
Marsolais GS, Dvorak G, Conzemius MG. (2002). Effects of postoperative rehabilitation on limb function after cranial cruciate ligament repair in dogs. Journal of the American Veterinary Medical Association, 220(9), 1325–1330.
Millis DL, Levine D. (2014). Canine Rehabilitation and Physical Therapy. 2nd ed. Elsevier.
Pozzi A, Kim SE, Banks SA, et al. (2013). Cranial cruciate ligament function and biomechanics in the dog. Veterinary Surgery, 42(2), 171–182.
Slocum B, Slocum TD. (1993). Tibial plateau leveling osteotomy for repair of cranial cruciate ligament rupture in the canine. Veterinary Clinics of North America: Small Animal Practice, 23(4), 777–795.
Vasseur PB. (2003). Clinical results following nonoperative management for rupture of the cranial cruciate ligament in dogs. Veterinary Surgery, 32(5), 463–466.
Warzee CC, Dejardin LM, Arnoczky SP, et al. (2001). Effect of tibial plateau angle on cranial cruciate ligament strain. Veterinary Surgery, 30(6), 687–693.
Witsberger TH, Villamil JA, Schultz LG, et al. (2008). Prevalence of and risk factors for hip dysplasia and cranial cruciate ligament deficiency in dogs. Journal of the American Veterinary Medical Association, 232(12), 1818–1824.



Comments